Also known as trabecular cell carcinoma of the skin, primary neuroendocrine carcinoma of the skin
What is Merkel cell carcinoma?
Merkel cell carcinoma is a very uncommon type of aggressive skin cancer. This type of skin cancer is caused when a particular type of skin cell grows out of control. It is most common in elderly fair-skinned individuals and is more common in men. It most often starts on sun-exposed areas on the head, neck, arms, and legs. In a small number of people, it is only diagnosed after it has already spread to a lymph node or another part of the body, without an initial skin lesion being detected.
Australia has the highest incidence of Merkel cell carcinoma in the world, with Queensland having the highest incidence. This is likely due to higher rates of UV exposure.
What causes Merkel cell carcinoma?
There are two known causes of Merkel cell carcinoma. One of these causes is UV radiation from sun exposure, which is the most common cause in Australia and New Zealand. The other main cause of Merkel cell carcinoma is the Merkel cell polyomavirus, which is a virus found on human skin. This virus has been found in up to 80% of Merkel cell carcinoma cases in the Northern Hemisphere,(1) making it the most common cause in that region. Studies have shown that Merkel cell carcinoma caused by the Merkel cell polyomavirus have a better prognosis compared to UV related Merkel cell carcinoma.
Decreased immune function is also thought to play a role in the development of this form of cancer. As a result, Merkel cell carcinomas occur more frequently in people who are older, have had solid organ transplants or in people with human immunodeficiency virus (HIV) or acquired immunodeficiency syndrome (AIDS). It is also seen in some people with haematological cancers (cancers relating to the blood) such as chronic lymphocytic leukaemia.
What does Merkel cell carcinoma look like?
Merkel cell carcinoma usually presents as a reddish to purplish lump which grows quickly, most often located in sun exposed areas, such as the head and neck. They are often non-tender and, in most cases, produce no other symptoms.
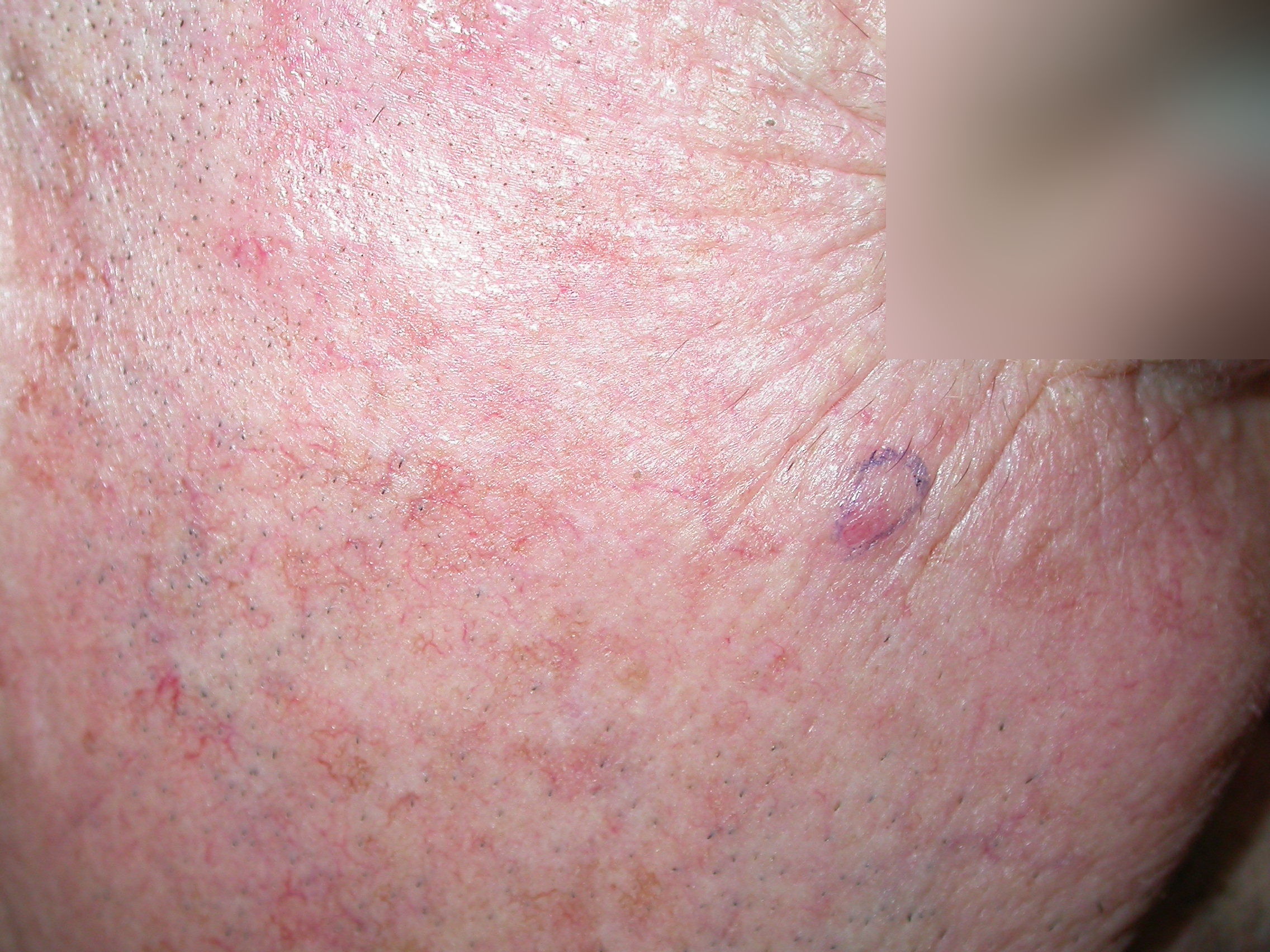
Figure 1. Image reproduced with permission of Dr Brian De’Ambrosis

Figure 2. Image reproduced with permission of Dr Brian De’Ambrosis
How is Merkel cell carcinoma diagnosed?
Merkel cell carcinoma can be difficult to diagnose because it can look like other types of skin cancers or cysts.
The dermatologist will thoroughly examine the skin to look for any signs of skin cancer. If a lump looks suspicious, a sample (biopsy) of it is taken to confirm the diagnosis under a microscope.
If the biopsy confirms that the suspicious lump is a Merkel cell carcinoma, additional tests may be done to find out if the Merkel cell carcinoma has spread to other parts of the body.
- The dermatologist will do another thorough physical examination to look for any indication that the cancer may have spread to other parts of the body, particularly focusing on the lymph nodes and abdomen.
- Diagnostic imaging tests may also be needed. These tests can include PET (position emission topography), CT (computed tomography) and MRI (magnetic resonance imaging) scans.
- A special test called a sentinel lymph node biopsy may be needed. This investigates the draining lymph nodes that the cancer may have spread to.
How is Merkel cell carcinoma treated?
Different types of treatments are available for patients with Merkel cell carcinoma. Treatment depends on whether the cancer has spread to other parts of the body, as well as individual considerations for each person.
Surgery is one of the main forms of treatment. This involves the Merkel cell carcinoma being surgically cut out, as well as a margin of normal skin surrounding the edge of the cancer to ensure that the cancer is entirely removed.
Radiotherapy is another form of treatment. This can be used in combination with other treatments, or as the only treatment method.
Chemotherapy may also be used if the Merkel cell carcinoma has already spread away from the first site where it was originally found.
Immunotherapy is another more recent effective form of treatment for treating Merkel cell carcinoma. Immunotherapy works by helping your body’s own immune system to fight the cancer.
What follow up is required?
People who have had a Merkel cell carcinoma will generally see their dermatologist every 3-4 months in the first 3 years and then if there are no signs of recurrence, less regular reviews are required. It is important to have regular full skin examinations to check for new cancers and monitor for signs of spread of the Merkel cell carcinoma.
What is the likely outcome of Merkel cell carcinoma?
The prognosis for Merkel cell carcinoma differs, depending on stage at diagnosis. Those who have small and localised tumours have a better prognosis than those whose disease has spread to local lymph nodes or other organs.
Merkel cell carcinomas also have a high chance of reoccurring in the original or different part of the body, which usually happens within the first 3 years of the first Merkel cell carcinoma being diagnosed. Recurrent disease generally has a lower survival rate.
Future developments
Researchers are currently investigating new ways that immunotherapy and somatostatin analogue drugs can be used for the treatment of Merkel cell carcinoma. Serology tests are currently being used overseas to detect antibodies against the Merkel cell polyomavirus to monitor people who have had a Merkel cell carcinoma caused by the Merkel cell polyomavirus. However, as Merkel cell carcinomas are primarily caused by UV radiation in Australia and New Zealand, this serology test is not currently being utilised in these countries.
Another form of therapy called Talimogene laherparepvec (TVEC), which is injected directly into a cancer on the skin, is also currently being studied for its effectiveness in treating Merkel cell carcinoma.(2)
References
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8212377/
- https://onlinelibrary.wiley.com/doi/10.1111/ajd.13881
This information has been written by Dr Georgia De’Ambrosis and Dr Brian De’Ambrosis
Last updated: December 2022