What is melanoma?
Melanoma is a cancer that arises in pigment cells of the skin (melanocytes). If not detected early, it has the capacity to spread through blood vessels and lymph channels to other parts of the body.
Australia has the highest rates of melanoma in the world. This is because of our sunny climate and fair skinned and mainly Celtic population. Melanoma is the most common cancer in Australians under fifty years of age and rates continue to increase. At least one in ten men and one in 16 women will develop a melanoma. Early diagnosis is essential to enable treatment before the melanoma spreads and becomes life threatening.
What causes melanoma?
There is overwhelming evidence that almost all melanomas are the result of previous sun exposure. Most melanomas in younger Australians (under 50 years) are due to occasional sun exposure of the kind that produces sunburn. Childhood sun exposure is a particularly important contributor to these melanomas. Melanomas in older Australians (over 50 years) are more strongly related to regular sun exposure over a long period.
What do melanomas look like?
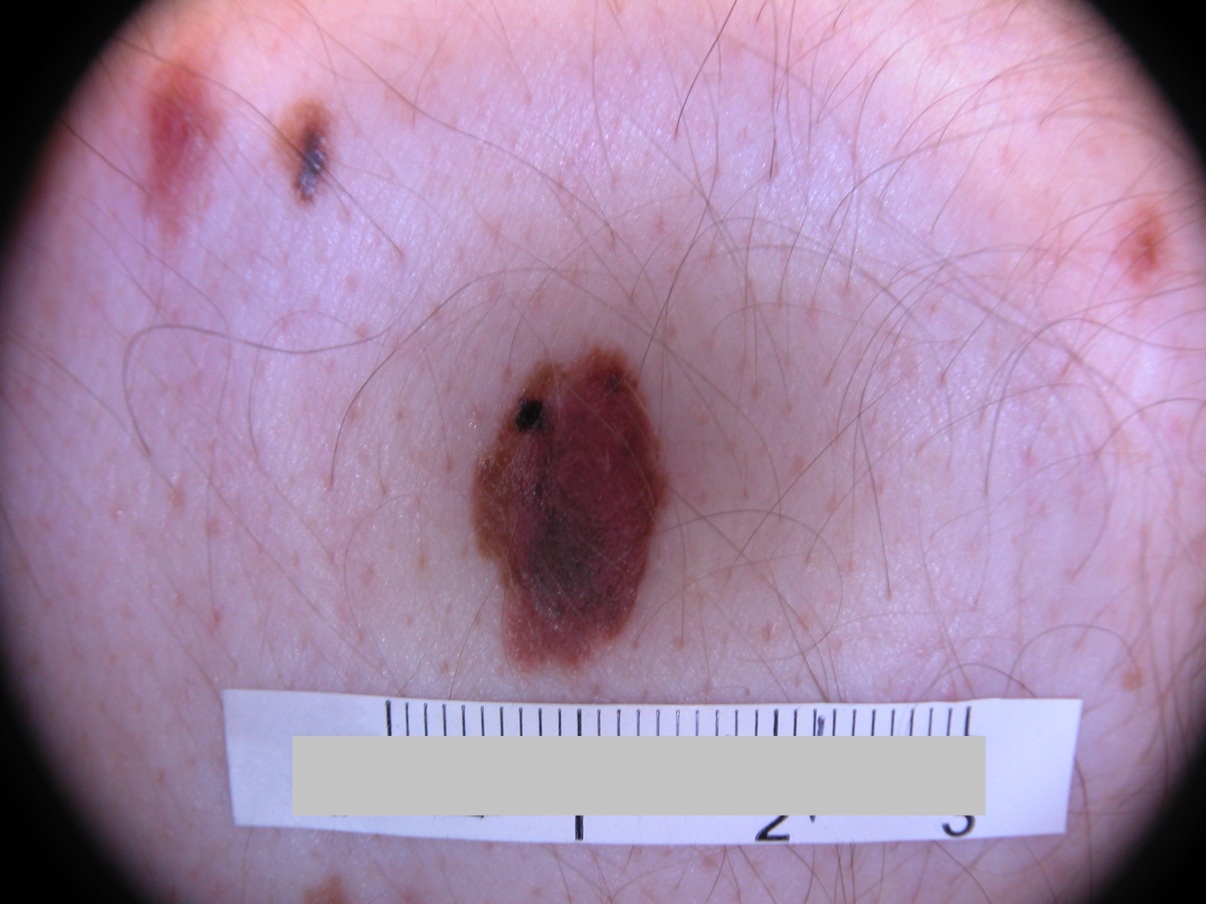
More than half of melanomas begin as a new spot and the remainder, arise from a pre-existing mole. They begin as a flat, light brown to black spot that looks like a mole. However, melanomas, unlike moles, will grow progressively larger at a rate that will often be detected over a few months. As they enlarge, changes in shape and colour also progress so that the spot becomes increasingly irregular in shape or variable in colour (Figure 1 and 2).
{kind=link}
{kind=link}
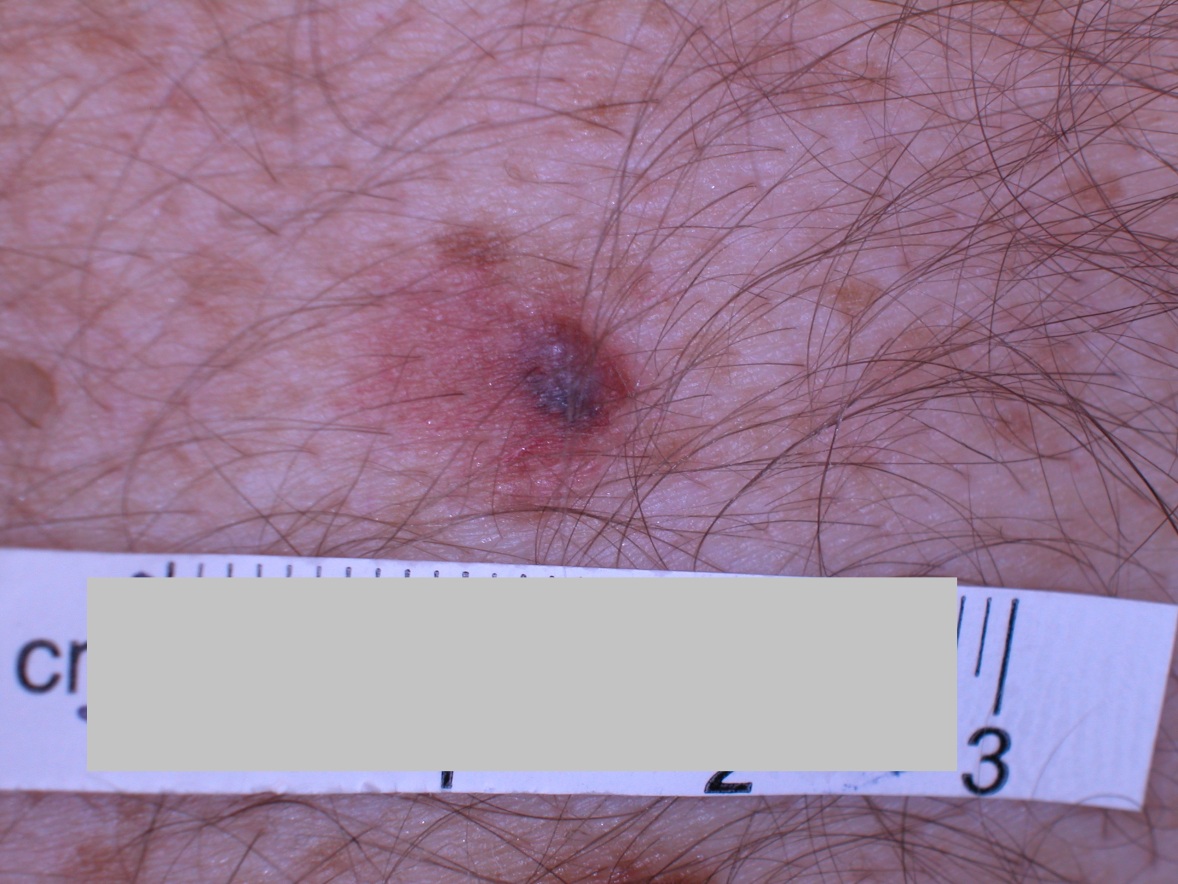
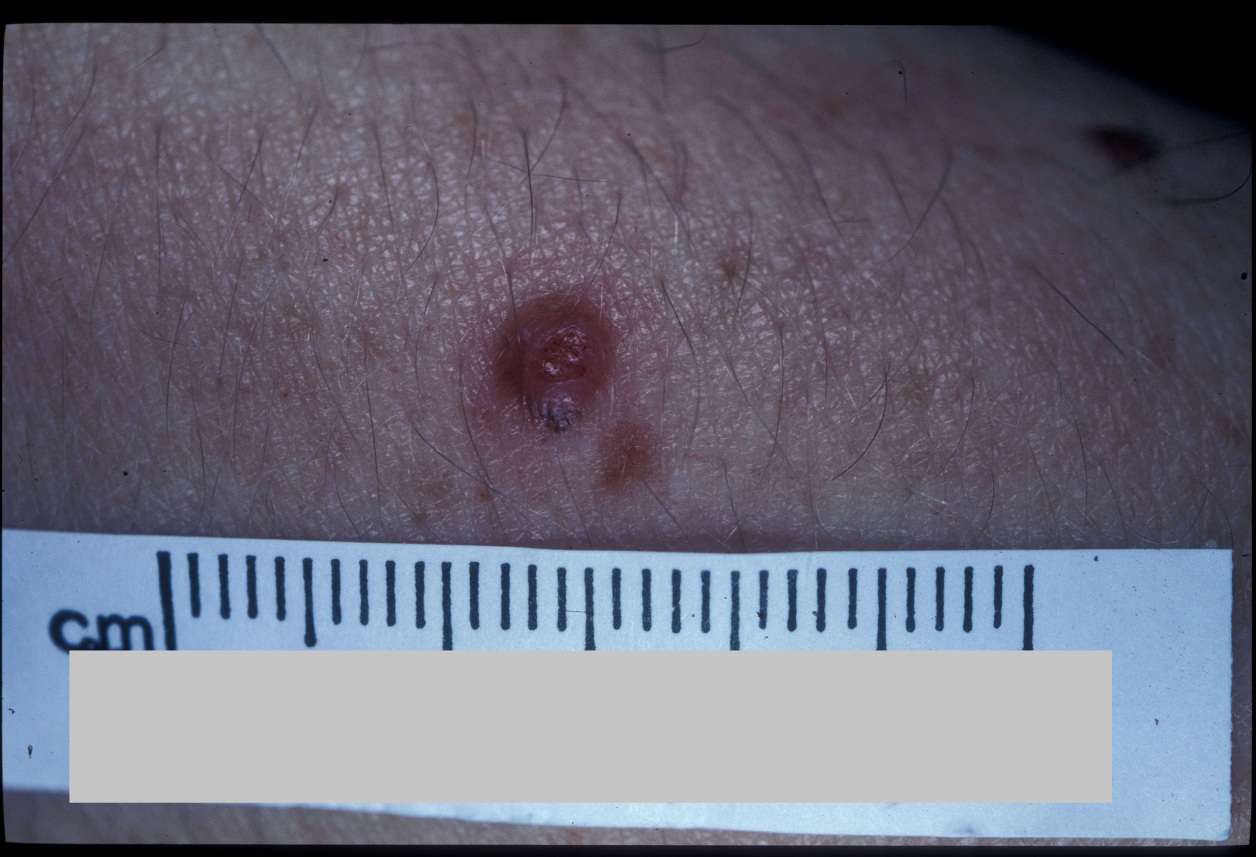
An important exception is the 20% of melanomas that have little or no pigment and appear predominantly red in colour (Figure 3).
{kind=link}
Another exception is nodular melanoma, which has no flat phase and presents as raised from the outset (Figures 4 and 5) and are also most often red in colour. These may bleed repeatedly especially if they are knocked or bumped.
{kind=link}
{kind=link}
Melanomas that are detected while they are still flat are almost always cured by removal. All melanomas will eventually become raised, increase in-depth and become more life threatening.
All Australians should check their own skin to look for changes, including parts of the body such as the back that are harder to see. It helps to have a partner or use two mirrors to examine your skin. A good way to remember is to check your skin at the beginning of each new season.
What other problems can occur with melanomas?
Melanomas are more common in people with fair skin. People with large numbers of moles or unstable (dysplastic) moles are more likely to develop a melanoma. Light hair (especially red hair) and light eye colour are associated with a greater risk of developing melanoma. Other risk factors include freckles (a marker of fair skin) and solar lentigines (sunburn freckles).
People who have had any kind of skin cancer are at higher risk and those who have already had a melanoma are at especially high risk (about 1% develop new melanomas each year). Those who have a close blood relative with melanoma have double the average risk.
People with strong risk factors for melanoma should be assessed regularly by a dermatologist.
How is melanoma diagnosed?
If you become suspicious about a spot, you should consult your GP. If the spot is obviously suspicious, it may be removed surgically, or you may be referred to a dermatologist urgently for assessment. If you have good reason to be suspicious, do not hesitate to question your doctor’s opinion and explain your reasons for concern. If possible, any suspicious spot should be removed completely and the entire spot sent to pathology for assessment. Partial biopsies can be unreliable for diagnosis but are sometimes necessary. When the pathology report is back, in a week or so, you will be told the result. The pathologist measures the depth of the melanoma in millimetres, and this is the most important determinant of the risk attached to it. At this stage, your doctor may explain the risk and the treatment options or refer you to an expert.
How is melanoma treated?
All melanomas are treated surgically by removing both the melanoma along with a safety margin of normal appearing skin around it.
The width of the safety margin removed varies according to the depth of the melanoma. If the melanoma is more than 0.8 mm in depth, there may be the option of a sentinel node biopsy. This procedure identifies the first lymph node that drains the site of the melanoma and then the lymph node is removed at the same time as a wider safety margin around the melanoma itself. If melanoma is present in the lymph node the risk of further spread of the melanoma is greater.
Sentinel node biopsy may provide information about your risk for spread of melanoma beyond the skin. In addition, for people with both a higher risk primary melanoma and a positive sentinel lymph node biopsy, the addition of targeted or immunotherapy will offer a reduced chance of recurrence
Treatment with drugs targeting specific melanoma mutations (targeted therapy) or immunotherapy will reduce recurrence after initial melanoma spread has been treated. These drugs are also used to treat advanced spread that cannot be surgically removed. These drugs have greatly improved the outlook after spread of melanoma has occurred.
What is the likely outcome of melanoma?
The life-threatening potential of a melanoma varies according to several key prognostic factors. Factors that affect your risk for further issues with spread from your melanoma include the depth of the melanoma (thickness), ulceration (surface breakdown and crusting), the rate of growth of your melanoma (mitotic rate) and the stage of your melanoma (how advanced and how far spread it already is).
Further information about melanoma
ACD, A-Z of Skin page, Skin cancer: An overview
Cancer Council Australia, Optimal Cancer Care Pathway for people with melanoma
This information has been written by A/Prof John Kelly
Last updated: October 2022
Disclaimer
2019 © Australasian College of Dermatologists.
You may use for personal use only. Please refer to our disclaimer.